
FieldStrength MRI magazine
User experiences - November 2016
When MRI is the preferred choice, ED patients can get fast MRI and fast diagnosis
When neurological emergencies require diagnostic imaging, common practice in the ED has been to perform CT rather than MRI, even when MRI could potentially produce more informative diagnostic images of spinal cord damage, disc protrusions, soft tissue injuries, and stroke pre-cursors. [1,2] The main reason is that timing is essential in emergency cases, and CT is generally faster than MRI. The St. Joseph’s Hospital and Medical Center is now challenging this paradigm by offering rapid MRI scans within its Neurologic ED and seeing that it helps them make a richer diagnosis.
“We're heading towards first time right imaging”

John Karis, MD
John Karis, MD, is a neuroradiologist and director of MRI and brain imaging at Barrow Neurological Institute at St. Joseph's Hospital & Medical Center in Phoenix, Arizona since the early 2000's. Dr. Karis completed his residency at the Duke University School of Medicine.
Introducing MRI in the ED: why the change?
“In the past, CT scans were performed because of their availability and rapid turnaround time” Dr. Karis argues, “but if an MRI could be as
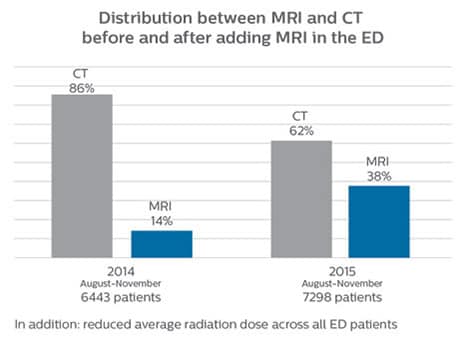
Since 2012, St. Joseph’s Hospital and Medical Center in Phoenix, Arizona, USA, has had an ED dedicated to neurological patients. In 2015, John Karis, MD, of the Barrow Neurological Institute at St Joseph’s spearheaded a project to place an MRI system in the Neuro ED. He stressed the added prognostic value of having an emergency MRI, and the importance of reducing radiation doses, particularly in patients for whom a CT scan was not the optimal test.
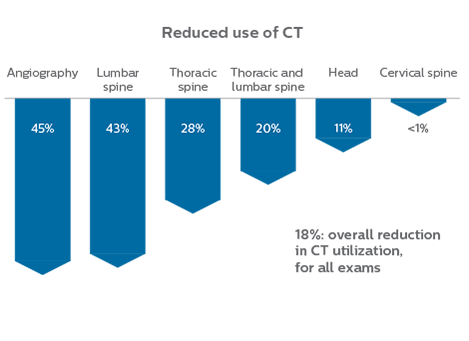
efficient as CT for referring physicians, then physicians would probably prefer MRI over CT in part of the cases. Reducing the number of CT scans for patients less than 40 years of age without significant acute findings, such as acute stroke, was also a main reason for introducing MRI into the ED. “MRI is a better test for identifying soft tissue abnormalities in the brain. What really influenced the decision on the administrative side, was the total radiation dose received by ED patients, and how this could be reduced by introducing MRI in the ED”.
Introducing MRI in the ED: why the change?
“In the past, CT scans were performed because of their availability and rapid turnaround time” Dr. Karis argues, “but if an MRI could be as efficient as CT for referring physicians, then physicians would probably prefer MRI over CT in part of the cases. Reducing the number of CT scans for patients less than 40 years of age without significant acute findings, such as acute stroke, was also a main reason for introducing MRI into the ED. “MRI is a better test for identifying soft tissue abnormalities in the brain. What really influenced the decision on the administrative side, was the total radiation dose received by ED patients, and how this could be reduced by introducing MRI in the ED”.
Since 2012, St. Joseph’s Hospital and Medical Center in Phoenix, Arizona, USA, has had an ED dedicated to neurological patients. In 2015, John Karis, MD, of the Barrow Neurological Institute at St Joseph’s spearheaded a project to place an MRI system in the Neuro ED. He stressed the added prognostic value of having an emergency MRI, and the importance of reducing radiation doses, particularly in patients for whom a CT scan was not the optimal test.
")
")
")
")
Towards routine scan times of about 10 minutes
in image acquisition and postprocessing algorithms.”“mDIXON TSE sequences allow simultaneous characterization of morphological changes from the in-phase T2-weighted images and visualization of edematous changes, thanks to the water T2-weighted images from the same acquisition. Anatomical and morphological considerations could be a partial or complete ligament tear, a bony avulsion or hematoma.” “For soft tissue assessment mDIXON brings similar benefits. For example in one T2-weighted mDIXON TSE acquisition, having the multiple contrasts helps us assess abnormalities in peripheral nerves fascicles, which may be due to anatomical or inflammatory changes..” “In peripheral joints, we get good image quality in difficult areas with mDIXON TSE. Fat suppressed images appear homogeneous over the entire image, even with large coverage at 3.0T – for instance in scapular or hip girdles – or in the bearing areas or around metal prostheses*, where fat suppression is often deficient with STIR or spectral fat suppression, causing diagnostic difficulties. If a diagnostic image is right the first time, we don’t need to repeat or add a sequence.” “mDIXON TSE sequences allow simultaneous characterization of morphological changes from the in-phase T2-weighted images and visualization of edematous changes, thanks to the water T2-weighted images from the same acquisition. Anatomical and morphological considerations could be a partial or complete ligament tear, a bony avulsion or hematoma.” “For soft tissue assessment mDIXON brings similar benefits. For example in one T2-weighted mDIXON TSE acquisition, having the multiple contrasts helps us assess abnormalities in peripheral nerves fascicles, which may be due to anatomical or inflammatory changes..”
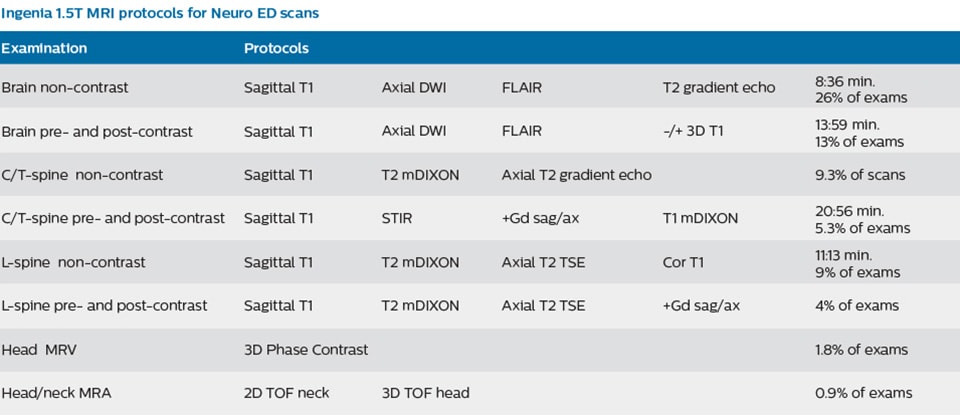
In order to address efficiency, matched with state-of-the-art capabilities to support a rich diagnosis, the decision was taken to include a Philips Ingenia 1.5T MRI scanner with wide bore in the new setup of the ED to enable scanning of virtually all patients.
To minimize the time taken to perform scans, rapid MRI examination protocols (ExamCards) were developed, shortening the total scanning time to even less than 10 minutes in some exams. Techniques like mDIXON (modified DIXON) are used for robust capturing of fat-free MRI images in a hectic ED environment.
“mDIXON is robust with regard to susceptibility type of problems that would come up with traditional spectral fat-saturated images.”

The Barrow Neuroscience Tower at St. Joseph's was opened in 2006.
“In our ED environment it’s really nice to have the fat-free imaging that goes along with the mDIXON technique.”
Including mDIXON TSE for robust fat suppression
“We use mDIXON TSE extensively in our spine imaging in the emergency room,” says Dr. Karis. “It’s particularly nice in that it is very robust with regard to susceptibility type of problems that would come up with traditional spectral fat-saturated images; these problems are essentially eliminated with the mDIXON technique. In our ED environment it’s really nice to have the fat-free imaging that goes along with the mDIXON technique.
“For the thoracic and cervical spine routine non-contrast exam, for example, we perform one mDIXON T2 TSE sequence, which provides us with two outputs: the fat-and-water-together T2-weighted images, as well as the water-only sagittal T2-weighted images. And then we also perform an axial gradient echo exam.”
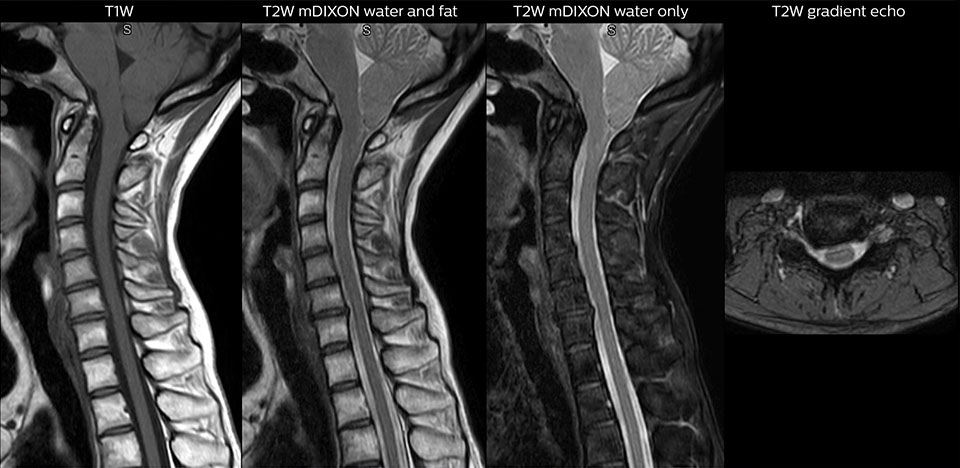
Cervical spine routine exam
This patient presented with headache that was worse with neck flexion and we see a Chiari 1 malformation with low-lying cerebellar tonsils as well as some degenerative cervical thrombolytic change.
Guidance on appropriate use of MRI
“For soft tissue assessment mDIXON brings similar benefits. For example in one T2-weighted mDIXON TSE acquisition, having the multiple contrasts helps us assess abnormalities in peripheral nerves fascicles, which may be due to anatomical or inflammatory changes..” “In peripheral joints, we get good image quality in difficult areas with mDIXON TSE. Fat suppressed images appear homogeneous over the entire image, even with large coverage at 3.0T – for instance in scapular or hip girdles – or in the bearing areas or around metal prostheses*, where fat suppression is often deficient with STIR or spectral fat suppression, causing diagnostic difficulties. If a diagnostic image is right the first time, we don’t need to repeat or add a sequence.” “mDIXON TSE sequences allow simultaneous characterization of morphological changes from the in-phase T2-weighted images and visualization of edematous changes, thanks to the water T2-weighted images from the same acquisition. Anatomical and morphological considerations could be a partial or complete ligament tear, a bony avulsion or hematoma.” “For soft tissue assessment mDIXON brings similar benefits. For example in one T2-weighted mDIXON TSE acquisition, having the multiple contrasts helps us assess abnormalities in peripheral nerves fascicles, which may be due to anatomical or inflammatory changes..”
A range of protocol sheets was developed to help ensure that referring physicians order the most appropriate MRI exam. The optimized MRI protocols also include 3D contrast-enhanced imaging, allowing neurosurgeons to comfortably use the isotropic data in the operating room while performing stereotaxic surgery.
After the MRI scanning, the preliminary reports are made available to referring physicians more quickly than before, because that is what physicians need to make their decision on what to do with patient. Using a redesigned reporting process results in total turnaround times that are similar to those of CT. Another of the changes introduced is that MRI safety screening data are retrieved from the hospital information system, saving approximately 30 minutes.

The MRI suite with Ingenia 1.5T
“The MRI scanner is available for targeted exams only. This requires referrers to think clearly about what they want to test.”
Changing established behaviors
The transition away from a predominantly CT-based ED began by educating physicians about the advantages of MRI in the emergency setting, when to use MRI, and the importance of targeted exams instead of broader, non-targeted exams. Some resistance to the change was anticipated, as it was disrupting established routines, so a reasonable amount of time was planned for educating referrers, neuroradiologists and neurosurgeons, as well as residents and fellows. However, less time than anticipated was needed: all involved were already familiar with MRI and, more importantly, they were easily persuaded on learning about the 10-minute exam duration with MRI.
“We bring forward that the MRI exam time is similar to CT, which is very important to them”, says Dr. Karis. “One of the other points to stress is that the MRI scanner is available for targeted exams only. This requires referrers to think clearly about what they want to test. There must be a true commitment to the shorter time frame; otherwise, the process won’t work.”
“Experienced neuroradiologists adapted fairly instantly – they knew the value of MRI and as such, quite quickly learned to use just the three or four sequences for their diagnosis. In fact, one came to me and asked ‘why don’t we do this for all of our patients, all the time?’ This is not realistic in our center, of course [e.g. because of issues relating to demand, availability, and the range of conditions dealt with] but it illustrates the confidence in the approach”.
“In my experience a negative MRI, because it is so sensitive to abnormality, far exceeds the value of a negative CT.”
The high value of a negative MRI scan
“One of the most important decisions an ED physician has to make is to admit or discharge their patient. So a physician who is better informed by an MRI exam can make this decision with more confidence. By converting to a test that has a far better potential to identify issues, physicians get a better and more certain diagnosis."
"In my experience a negative MRI, because it is so sensitive to abnormality, far exceeds the value of a negative CT. A negative MRI can allow physicians to be more confident about making discharge decisions, potentially reducing the number of admissions in cases of doubt, and offering cost savings for the institute."
“There are far more decisions being made to send people home than to admit. And in terms of making that decision, I believe there’s no more valuable exam than a negative MRI for neurologic disorders.”
“The only unforeseen challenge,” says Dr. Karis “was the tendency to still perform non-targeted exams, particularly among less experienced staff and new neurology or neurosurgery residents. Since MRI image quality is so excellent, it’s just easier to ask for a number of tests, and then your exam goes from in and out in 10 minutes to much longer.”
Targeted scanning is important
The ED physicians can only request exams from a selected set of available exam protocols – as represented on the protocol sheet – minimizing the time necessary for the MRI scan. The sheet contains advice as to which scan to order (i.e. MRI vs. CT, contrast vs. non-contrast) depending on the situation, and encouraging physicians to order targeted scans. Even though the process has now been implemented, education still remains important; new neurology residents, for example, are informed as to the use of the ED MRI scanner, how it’s being utilized, and the importance of targeted scanning. “In my opinion, education has been crucial to establish the MRI exam as an ED test,” says Dr. Karis. “This is really key. If you can’t establish this concept, then you can’t convert everyone to the mindset that this is an ED test.”
“We're heading towards first time right imaging”
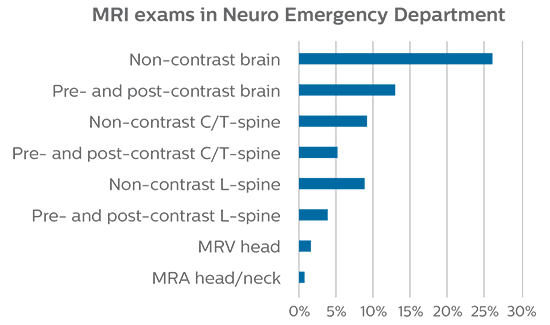
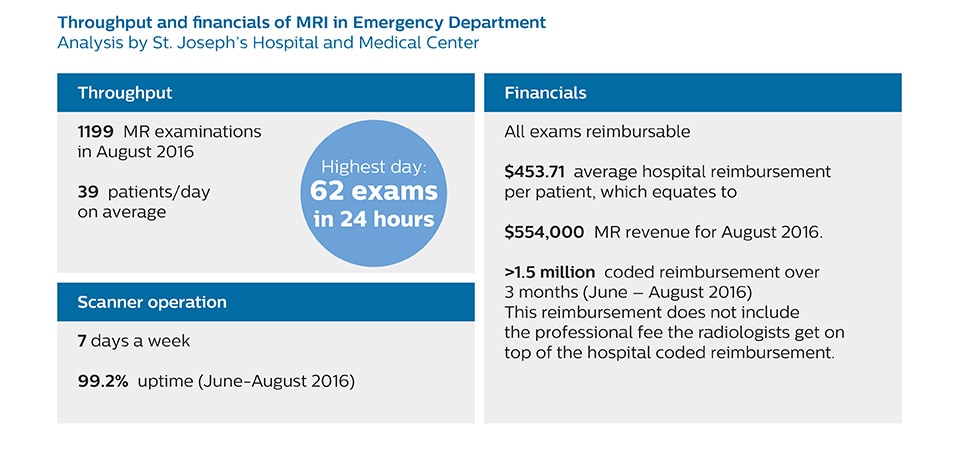
Growth of MRI in the Neuro Emergency Department
Patient turnaround times on par with CT
“Before, when patients received CT in the ED, it was quite common that they would need an MRI afterwards. However, in the four months that I have logged data for this study, I have not become aware of a single patient that underwent MRI in the ED and had to come back for repeat imaging, probably because the protocols are so robust. Patients with complicated cases requiring specialty acquisition types are the most common reason for recalls at our institution.”
“Our results show that a dedicated MRI in the ED can be effectively implemented; patient turnaround times with MRI were on par with CT. Interestingly, even though the MRI exam protocols were shortened, this robust yet rapid scanning still yielded good quality images, further improving our workflow and almost eliminating the need for repeat scans or follow-up scans. So, we’re heading towards first time right imaging,” says Dr. Karis.
“In the four months that I have logged data for this study, I have not become aware of a single patient that underwent MRI in ED and had to come back for repeat imaging.”
How to achieve a successful transition?
The successful incorporation of MRI into the ED is dependent on several factors, according to Dr. Karis. “First, it is necessary to have the MRI in close proximity to the ED, bypassing the need for hospital staff to leave the ED for extended periods in order to accompany patients to other departments. Also, exams must be streamlined, so that they can be performed in about 10 minutes or less. Targeted scans should be ordered for the specific issue at hand, and non-targeted exams should be discouraged. In particular, neurology and neurosurgery residents who work
overnight shifts should understand the shortened protocols, in the effort to avoid ordering extra scans that could extend exam times and hinder workflow.” Dr. Karis recommends that a global view should be considered before the change can be implemented. “You need to look at everything, from metal screening and nursing, to transport and proximity to the ED, if you’re really going to make this transition successfully.”
How to achieve a successful transition?
The successful incorporation of MRI into the ED is dependent on several factors, according to Dr. Karis. “First, it is necessary to have the MRI in close proximity to the ED, bypassing the need for hospital staff to leave the ED for extended periods in order to accompany patients to other departments. Also, exams must be streamlined, so that they can be performed in about 10 minutes or less. Targeted scans should be ordered for the specific issue at hand, and non-targeted exams should be discouraged. In particular, neurology and neurosurgery residents who work overnight shifts should understand the shortened protocols, in the effort to avoid ordering extra scans that could extend exam times and hinder workflow.” Dr. Karis recommends that a global view should be considered before the change can be implemented. “You need to look at everything, from metal screening and nursing, to transport and proximity to the ED, if you’re really going to make this transition successfully.”
"You need to look at everything, from metal screening and nursing, to transport and proximity to the ED, if you’re really going to make this transition successfully.”
Future plans: expansion to stroke and TIA patients
At St. Joseph’s Hospital and Medical Center, the dedicated MRI system in the ED has been shown to efficiently provide high quality MR images that assist physicians in making informed decisions on patient diagnoses and take a more definitive decision on follow-up. The decision to have a dedicated ED MRI has resulted in rapid patient turnaround, efficient patient management, and substantial reductions in radiation dose.
For Dr. Karis, the next goals for the neuro ED include converting the exams for acute stroke and TIA patients from CT to MRI, offering an alternative management option for these patients. Also, collaboration between other departments is currently underway, encouraging the performance of targeted exams with the ED MRI. These improvements in workflow and faster turnaround times may result in further reductions in scanning time.
2. Grimm JM, Schindler A, Schwarz F, Cyran CC, Bayer-Karpinska A, Freilinger T, Yuan C, Linn J, Trelles M, Reiser MF, Nikolaou K, Saam T. Computed tomography angiography vs 3 T black-blood cardiovascular magnetic resonance for identification of symptomatic carotid plaques. J Cardiovasc Magn Reson. 2014;16:84.
References
1. Singh R, Kumar RR, Setia N, Magu S. A prospective study of neurological outcome in relation to findings of imaging modalities in acute spinal cord injury. Asian J Neurosurg. 2015;10:181-9.
Results from case studies are not predictive of results in other cases. Results in other cases may vary.
"There must be a true commitment to the shorter time frame; otherwise the process won't work.”
Clinical cases
More from FieldStrength